Although it is one of the most crucial duties in nursing practice, documentation is also one of the most difficult and perplexing assignments for nursing students. Many students place a lot of emphasis on clinical skills like observations, wound care, and injections, but they often underestimate the severity of documentation errors. Nursing documentation is not only a university requirement in Australia, but also a legal record. Patient safety, professional accountability, and even legal results can be directly impacted by what you write—or don’t write.
Nursing students frequently experience documentation anxiety because they are unsure of what is permissible, what terminology to use, and what should never be recorded. Seldom are frequent mistakes, harmful blunders, and even minor phrasing choices can drastically alter a note’s meaning explained to students. This essay closes that gap by outlining the most typical documentation errors made by nursing students and demonstrating how to produce legally sound, safe, and professional notes while on placement.
This manual, which was created specifically for Australian nursing students—including those from other countries—uses straightforward language that is simple to comprehend and implement on the ward.
1. Why Documentation Matters More Than Students Realise
A common misconception among nursing students is that documentation is merely “writing what happened” or something completed hastily at the conclusion of a shift. Documentation is actually a formal means of communication between medical experts. Nursing notes may be read by physicians, nurses, allied health personnel, auditors, and legal teams.
In Australia, paperwork is frequently examined first when medical treatment goes awry. Even if the care was appropriate, the nurse may be held accountable if it is insufficient, ambiguous, emotional, or inaccurate. Inadequate documentation might result in academic warnings, job worries, or placement failure for students.
Patient safety is also directly impacted by documentation. In addition to preventing prescription errors and ensuring continuity of treatment, clear notes also assist personnel in understanding patient changes. Writing safe notes is not about using fancy language—it is about being clear, objective, factual, and respectful.
2. What NOT to Write in Nursing Documentation (Very Common Student Errors)
Writing things that shouldn’t be in patient notes is one of the most common errors made by nursing trainees. This sometimes occurs as a result of students writing informally, emotionally, or in an attempt to justify themselves rather than recording patient care.
Never write judgments, presumptions, or opinions on a patient. It is improper and unprofessional to write things like “patient is lazy,” “patient is rude,” or “patient exaggerates pain.” These claims can be damaging and are subjective.
Additionally, students erroneously record feelings of annoyance or anger, such as “patient was annoying,” “patient kept pressing the bell,” or “patient refused care again.” These expressions don’t represent patient behavior, but rather the sentiments of the staff.
Documenting blame is another grave error. Writing “nurse forgot,” “doctor did not come,” or “physio didn’t attend” might lead to legal trouble and professional difficulties. The focus of documentation should be on what transpired rather than who failed.
Additionally, students should never use sarcasm, humor, or personal remarks in their notes. Everything entered is a part of a permanent medical record, despite the informal nature of documentation methods.
Only patient treatment, patient response, and activities are covered in safe documentation.
3. Objective vs Subjective Language: A Critical Skill Students Struggle With
Safe nursing documentation requires an understanding of the distinction between objective and subjective terminology. Unknowingly, a lot of pupils confuse the two.
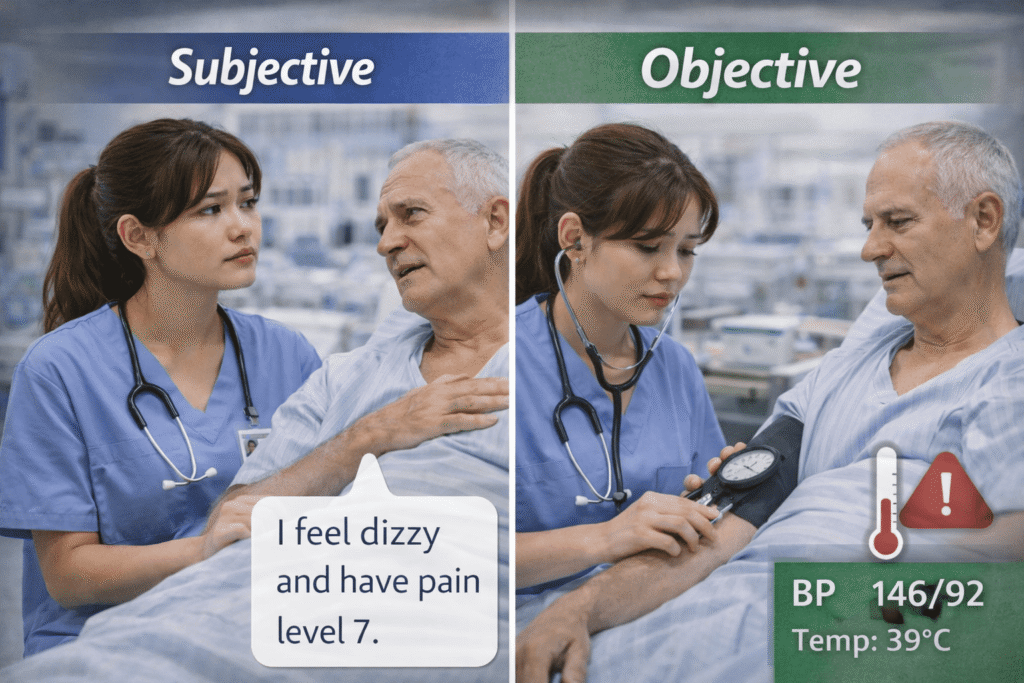
What the patient says is subjective information. It contains the patient’s stated symptoms, sentiments, and descriptions of their discomfort. For instance, “patient reports feeling dizzy” or “patient states pain is 7/10.”
What you can see, measure, hear, or evaluate is considered objective information. Vital indicators, bodily observations, and outward behavior are all included in this. For instance, “wound dressing dry and intact,” “blood pressure 140/90,” or “patient ambulated 10 meters with assistance”
Converting subjective impressions into objective statements is a typical error made by students. Unless there is proof, writing “patient is anxious” is subjective. “Patient pacing, wringing hands, and states feeling anxious” might be a more secure version.
Writing conclusions rather than observations is another error. “Patient had a panic attack,” for instance, is a diagnosis rather than an observation. A safer note would explain reported symptoms and behavior without labelling.
Safe documentation makes a clear distinction between the nurse’s observations and the patient’s words.
4. Confidentiality Errors Nursing Students Don’t Realise They Are Making
One of the most important documentation errors that nursing students commit, frequently without realizing it, is a breach of confidentiality. Students are subject to the same standards as registered nurses, and patient privacy is carefully protected by Australian healthcare regulations.
Incorrect use of patient identifiers is one frequent mistake. If personal notes, study materials, or reflective journals are not secure, writing complete names, dates of birth, or bed numbers may violate confidentiality.
Documenting needless personal information is another error. Only when it is therapeutically relevant should information about social behavior, lifestyle choices, or family conflict be recorded. Writing too much personal information raises the chance of privacy violations.
Outside of the clinical setting, students occasionally talk about documentation. Even without names, discussing patient notes with friends, classmates, or on social media might still indirectly identify patients.
Another major mistake is accessing patient records without a clinical justification. Only data pertaining to the patients they are caring for may be recorded or viewed by students.
One guideline governs safe documentation: just write what is required for patient care, and make sure it is factual and professional.
5. Common Documentation Style Mistakes That Can Get Students in Trouble
Many problems with documentation are related to note-taking style rather than content. Students frequently have poor structure, inconsistent scheduling, and missing information.
Writing notes too late is a common error. As soon as care is given, documentation needs to be finished. There is a greater chance of losing information or making false claims when writing hours later.
Vague phrasing is another problem. “Patient okay,” “care done,” and “no issues” are examples of phrases that don’t offer any helpful information. Documentation needs to be quantifiable and precise.
Additionally, students neglect to record their follow-up actions. For instance, it may appear as though nothing was done if a concern is noted without recording who was notified or what was done.
Another concern is misusing acronyms. You should only use approved clinical abbreviations. Uncertain or informal acronyms may be misinterpreted and lead to mistakes.
Both the patient and the learner are protected by timely, organized, and clear documentation.
6. How to Write Safe, Professional Nursing Notes as a Student

The ability to write safe nursing notes gets better with practice. Documentation must be factual, straightforward, and patient-centered.
Documenting the rationale for care should come first. Next, note what you saw, what the patient said, what you did, and how the patient reacted. When necessary, always add the time, date, and your student designation.
Make use of impartial wording. Describe visible facts rather than making dramatic or emotional claims. For instance, substitute “patient crying, raised voice, states feeling overwhelmed” for “patient extremely upset.”
Note that supervision was given if something falls outside of your purview. This demonstrates safe behavior and protects you.
Read your notes as though someone else would evaluate them later, as they probably will, before submitting or finalizing them.
7. Final Thoughts: Documentation Is Part of Patient Safety
Documentation is more than just paperwork. It is a fundamental nursing duty and a talent that you will need throughout your career. Early adoption of safe documentation practices will shield you as a student from stress, errors, and even disciplinary problems.
You don’t need to use complicated language or flawless grammar. You require professionalism, honesty, and clarity. When in doubt, make sure your notes are pertinent, courteous, and factual.
Safe paperwork demonstrates your training as a safe nurse.
People Also Ask
1. Can nursing students get in trouble for poor documentation?
Yes. Poor documentation can lead to placement failure or professional concerns.
2. Should students document emotions or opinions?
No. Only objective observations and patient-reported statements should be recorded.
3. Is it okay to write notes later in the shift?
Documentation should be completed as soon as possible to ensure accuracy.
4. What if I’m unsure how to document something?
Ask your preceptor or clinical facilitator for guidance.
5. Are students legally responsible for what they document?
Yes. Student documentation is part of the legal medical record.
Useful Documents for every Nursing Student
CV Section Template for Nursing students
AHPRA – NMBA Registration Document Checklist (International Students-Graduates)
Clinical Placement Reflection Template (NMBA-aligned)
Cover Letter Template for Nursing Students
Disclaimer: “I researched this information on the internet; please use it as a guide and also reach out to a professional for assistance and advice.This information is not medical advice, so seek your medical professional’s assistance.”