
Nursing care plans are essential tools in the healthcare system that provide a roadmap for the delivery of individualized patient care. These plans are created by nurses to identify patient needs, outline nursing interventions, and evaluate patient outcomes. A well-structured nursing care plan ensures continuity of care, enhances communication among healthcare providers, and supports evidence-based nursing practices.
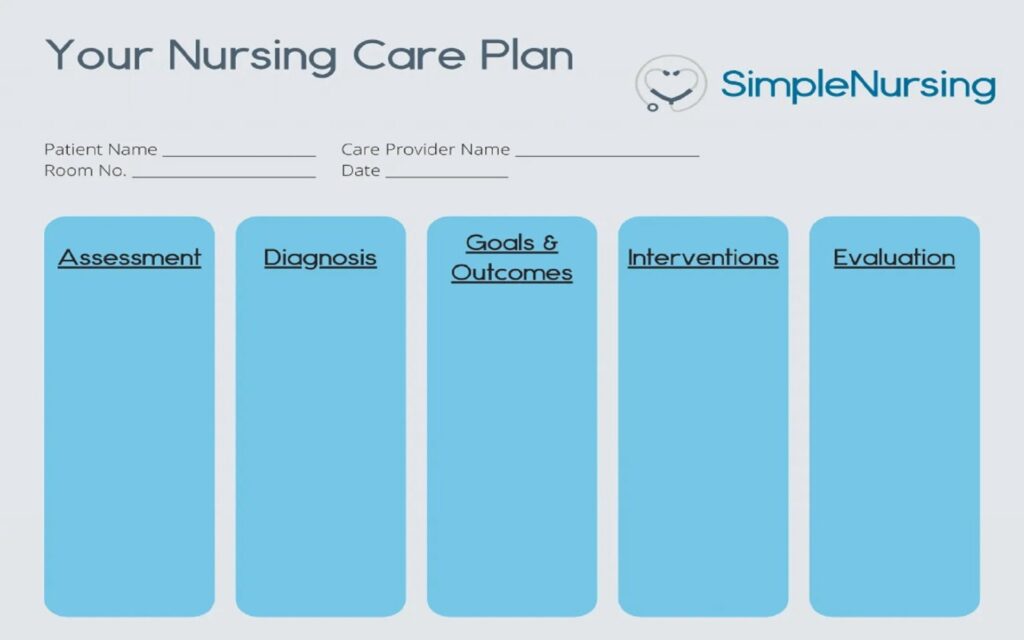
Nursing care plans are typically written using the nursing process, a five-step framework consisting of assessment, diagnosis, planning, implementation, and evaluation (ADPIE). Each phase is critical in delivering holistic and patient-centered care.
Importance of Nursing Care Plans
- Individualized Patient Care: Tailored interventions based on the patient’s unique health condition.
- Improved Communication: Standardizes care and enhances communication among team members.
- Legal Documentation: Serves as evidence of nursing care provided.
- Quality Assurance: Supports audits and quality improvement initiatives.
- Education and Research: Assists in training nursing students and conducting clinical research.
Components of a Nursing Care Plan
A nursing care plan includes the following key components:
- Assessment Data (Subjective and Objective)
- Nursing Diagnosis (Using NANDA-approved terminology)
- Goals and Outcomes (Short-term and long-term)
- Nursing Interventions (Independent, dependent, collaborative)
- Rationale for Interventions
- Evaluation Criteria
Nursing Care Plan Example: Patient with Congestive Heart Failure (CHF)
1. Assessment
Subjective Data:
- Patient reports shortness of breath while lying down (orthopnea).
- States feeling fatigued with minimal exertion.
- Complains of swollen feet and legs (edema).
- Reports waking up at night due to difficulty breathing (paroxysmal nocturnal dyspnea).
Objective Data:
- Blood pressure: 145/90 mmHg
- Heart rate: 110 bpm
- Respiratory rate: 24 breaths/min
- Bilateral pitting edema (+2)
- Oxygen saturation: 90% on room air
- Crackles heard in lower lung fields upon auscultation
- Weight gain of 2.5 kg over the past 3 days
2. Nursing Diagnosis
- Impaired gas exchange related to alveolar-capillary membrane changes as evidenced by crackles in lungs, SpO2 90%, and dyspnea.
- Decreased Cardiac Output related to altered contractility as evidenced by fatigue, edema, and increased heart rate.
- Excess Fluid Volume related to compromised regulatory mechanisms as evidenced by weight gain and pitting edema.
3. Goals and Expected Outcomes
Short-Term Goals (within 48 hours):
- Patient will maintain oxygen saturation ≥ 94% on supplemental oxygen.
- Patient will verbalize reduced shortness of breath.
- Patient will show reduction in peripheral edema.
Long-Term Goals (within 1 week):
- Patient will demonstrate improved activity tolerance.
- Patient will maintain stable weight.
- Patient will follow prescribed fluid and sodium restrictions.
4. Nursing Interventions and Rationale
Intervention 1: Monitor respiratory status and oxygen saturation every 4 hours.
- Rationale: Early detection of respiratory compromise allows prompt intervention to prevent hypoxia.
Intervention 2: Administer supplemental oxygen as prescribed.
- Rationale: Increases oxygen delivery to tissues and reduces the work of breathing.
Intervention 3: Position patient in high Fowler’s position.
- Rationale: Improves lung expansion and reduces venous return to the heart, easing breathing.
Intervention 4: Monitor intake and output, and daily weight.
- Rationale: Tracks fluid retention and evaluates effectiveness of diuretic therapy.
Intervention 5: Administer diuretics as prescribed and monitor electrolytes.
- Rationale: Promotes excretion of excess fluid, reducing edema and cardiac workload.
Intervention 6: Educate patient about low-sodium diet and fluid restriction.
- Rationale: Reduces fluid retention and helps manage heart failure symptoms.
Intervention 7: Encourage energy-conserving techniques and rest periods.
- Rationale: Prevents fatigue and promotes healing.
5. Evaluation
- Patient reports decreased shortness of breath and is able to speak in full sentences.
- Oxygen saturation improved to 95% on 2L nasal cannula.
- Edema reduced to +1 and weight decreased by 1 kg.
- Patient demonstrates understanding of fluid restriction and sodium limitation.
Common Nursing Diagnoses and Care Plans
Here are examples of common nursing diagnoses and brief interventions:
1. Acute Pain
- Assessment: Patient reports pain 8/10 postoperatively.
- Interventions: Assess pain every 2 hours, administer analgesics as prescribed, provide comfort measures.
- Goal: Pain reduced to ≤3/10 within 1 hour of intervention.
2. Risk for Infection
- Assessment: Surgical incision with slight redness.
- Interventions: Monitor temperature, assess wound daily, maintain sterile dressing changes.
- Goal: No signs of infection throughout hospital stay.
3. Ineffective Airway Clearance
- Assessment: Productive cough, wheezes on auscultation.
- Interventions: Encourage coughing and deep breathing, administer bronchodilators.
- Goal: Patient maintains clear lung sounds within 48 hours.
Developing Critical Thinking in Nursing Care Plans
Creating a care plan is not a simple checklist activity. It requires critical thinking, clinical judgment, and patient collaboration. Nurses must:
- Prioritize patient problems.
- Recognize changes in condition.
- Adjust plans based on outcomes.
- Incorporate interdisciplinary input.
- Document accurately and thoroughly.
By integrating critical thinking, nurses ensure that the care plan is dynamic, responsive, and centered around the patient’s goals and needs.
Challenges in Nursing Care Planning
1. Time Constraints
Many nurses face heavy workloads, limiting the time available to write comprehensive care plans.
2. Inadequate Training
Some nursing students and new nurses struggle with applying theoretical knowledge to real-life care plans.
3. Changing Patient Conditions
Patient status can evolve rapidly, requiring continuous updates to care plans.
4. Electronic Health Records (EHRs)
While EHRs streamline documentation, pre-filled templates may lead to generalized care plans instead of individualized ones.
Strategies to Improve Nursing Care Plans
- Use standardized nursing languages like NANDA, NIC (Nursing Interventions Classification), and NOC (Nursing Outcomes Classification).
- Encourage collaboration between nurses and other healthcare team members.
- Conduct care plan workshops and simulations.
- Regularly update care plans based on patient progress.
- Foster reflective practice through clinical debriefings.
Conclusion
Nursing care plans are foundational to quality nursing practice. They serve not only as guides for delivering care but also as tools for improving patient outcomes, promoting safety, and ensuring accountability in nursing practice. By using a systematic approach like the nursing process, incorporating evidence-based interventions, and continuously evaluating patient responses, nurses can deliver holistic and effective care. Whether caring for a patient with congestive heart failure or managing post-operative pain, a well-structured nursing care plan reflects the art and science of nursing at its best.
Disclaimer:
“I researched this information on the internet; please use it as a guide and also reach out to a professional for assistance and advice. This information is not medical advice, so seek your medical professional’s assistance.”